We are only just beginning. We started with a vision about wanting to share the best practices that we are seeing in our facilities throughout the organization. With a centered focus on long-term care, we turned our vision into reality with the creation of the LTC Think Tanks. Below you will read a brief recap about a few of our LTC Think Tanks, and we hope to continue to bring you innovative, inspiring, passion-driven ideas to help keep your long-term care residents performing at their highest level of potential with the ultimate goal to decrease their risk of further decline.
If you or members of your team would like support in program development, patient care identification strategies, and/or feedback on questions regarding long-term care, please reach out to LTC_TaskForce@ensignservices.net. Our mission is to provide a centralized hub to facilitate the dissemination of ideas.
Renew Purpose and Restore Peace
The rehab team at the Garrison facility, led by Christa Keesee, is inspiring us all. By identifying the needs of their patients, they created a specialized program to “Renew Purpose and Restore Peace” for their ever-deserving long-term care residents. Molly Setliff, occupational therapist from Garrison, provided a thorough presentation to help walk you through the mission and implementation process of the program. Molly also takes you through challenges you may experience and helpful alternatives.
Reach out to Christa Keesee to learn more.

Benefits of Using Therapy Animals in LTC
We had great contributors such as Michelle Wang, Jon Anderson, Barbara Mohrle and Ciara Cox who centered on the benefits of using therapy animals in LTC. Each has had great experience with using therapy animals in their facilities, and it provided great joy to many of the patients during their treatment sessions. We have a detailed presentation that bullets the ADL and musculoskeletal benefits of using therapy animals during patient care.
If considering a pet therapy program, consult with your state to ensure you have all requisite elements in place and also that the facility has a policy in place, as the state will look for this on survey.
Below are some helpful sites to visit if you are interested in learning more about therapy animals or getting your animal trained:
- Take a look at the Good Dog Citizen program at https://www.akc.org/ to learn more about the specialized training program.
- Contact your local zoo. Many are available to come on site and visit your facilities with a variety of animals.
- Search Google under Therapy Animals along with the name of your city. This search will populate contacts for therapy animals in your area.
…But How Should I Document
We usually receive tons of questions regarding how to best document our skilled maintenance services that are provided to our LTC patients. A special thank-you to Lori O’Hara for debunking some documentation myths surrounding Skilled Maintenance Therapy and for also giving us clear breakdowns of what this type of service should look like. We offer a skilled Maintenance POSTette, located on the portal, which includes documentation examples.
During the Think Tank, we also shared a really cool therapy tracking tool. The creator, Shaun Baldwin, was unable to join us, so I hope I did it justice with my explanation. We viewed the spreadsheet, which has a ton of information; he uses it during his Medicaid meetings to keep track of patients during the week. To make sure that he does not overlook any of his LTC residents, he built a section that lets him know how long it has been since a discipline last treated a patient. If the patient has not been on a discipline for longer than 75 days, the cell will turn yellow, and if it has been greater than 150 days, the cell will turn red. He uses the spreadsheet as a visual reminder of who may need to receive a follow-up by therapy. Shaun is very open and available to answer any of your questions regarding the tracking tool. Shaun Baldwin is the DOR at our San Marcos facility in Texas.
Functional Jobs Program
Program development is not always about structured exercise programs and textbook balance training. There are a variety of programs that may not sound like therapy in the traditional sense, but they are oftentimes the most beneficial to our patients’ physical and psychological well-being. Do your residents need a “job”? Barbara Mohrle, DOR/Therapy Resource, and Marisa Parker, DOR/Therapy Resource, reminded us all about living a purposeful life and why that is so important to our residents.
What is the Functional Jobs Program? It is a LTC program designed to allow residents an opportunity to serve and take part in daily activities that keep them fulfilled.
- The therapy team realized that many of their residents had a passion to serve, and they wanted to take part in daily activities that allow them to improve/maintain their level of functional mobility and decrease the risk of injury.
- As therapists/assistants, we have an opportunity to provide skilled care to our patients and help prepare/engage them in their “job.”
Reach out to Barbara Mohrle and Marisa Parker for more information on implementing the Functional Job Program in your facility.
PTNM and NMES
Marci Williams, PT, DPT, and Katie Kellagher, CCC-SLP, discussed two types of modalities that can significantly impact a patient’s quality of life.
Here are some key takeaways:
Percutaneous Tibial Neuromodulation (PTNM)
- Geared toward patients suffering from urinary incontinence
- Huge opportunity for the therapy and nursing partnership
- Email LTC_Taskforce for assistance with implementation
- This is a service-based billing code with opportunity to provide care to more than one patient at a time
Neuromuscular Electrical Stimulation (NMES)
- Certification in Vital Stim or NMES is a great adjunct to traditional interventions
- Referral sources are always excited to hear about therapists who are certified in NMES
- Please reach out to Elyse Matson, SLP Educational Resource, for additional support in modality implementation and/or documentation
Figuring Out LTC
Jennifer Kuehn, DOR from the Endura Market, led an excellent presentation on how to effectively navigate the area of LTC. Jenny dove into the clinical decision-making and patient identification process with great strategy and clinical reasoning. Reach out to Jenny to get your hands on her PowerPoint presentation. We received tons of great questions on the call; one question in particular stood out regarding patient weight loss. Elsye Matson, MA CCC-SLP, serves as our SLP educational resource. Elyse, with great detail, answered the posed question below. Please feel free to follow up with Elsye directly for further clarification.
What is the desired weight loss that a patient must have to warrant speech to evaluate?
SLPs should either be a part of the weight-loss committee or get updates from the RD in their facility on a weekly basis. The MDS triggers issues with weight loss at 5.0, 7.5, or 10.0% weight loss over a period such as a week or a month. There are a multitude of reasons one loses weight, including issues with self-feeding (refer to OT), medical complications affecting appetite and desired weight loss. A small amount of weight loss may indicate a serious issue if the patient was admitted weighing 80 pounds. Alternatively, a large weight loss from a 300-pound patient may be desired.
Finally, it is important to know information about meds, labs and conditions to differentiate a patient losing weight from diuresis/CHF issues versus true weight loss. So the circuitous answer re: weight loss and dysphagia is that it depends on each individual situation. We must always look at the whole patient and assess what is needed. There really is no correct answer, as weight loss is one symptom of many problems. We need to know our residents, stay in contact with our IDT and re-assess tube feedings and modified diets on a regular basis.
How Culture and Clinical Meet Financial
We had a great speaker by the name of Karlena (Valerie) Brooks, COTA. Karlena joined the Legend North Austin team as the Therapy Program Manager almost a year ago. Through her focus on revamping the culture and implementation of clinical programs, Karlena has tremendously grown her financial results in the area of LTC. It was wonderful to have her ED, Jocelyn, contribute to the discussion by sharing the effectiveness of what the development of a true partnership with the IDT can lead to. Reach out to Karlena to learn more; it will be well worth your time.
By Kai Williams, Therapy Resource

 cer. One of her goals is to get stronger to be able to tolerate a chemotherapy treatment regimen. The team’s new COTA, Jay, decided to try HRV training to reduce pain and increase function. During the first session, the patient was able to briefly get into what is called neurological coherence, as indicated on the biofeedback device as the green zone. However, the pain quickly brought her out of coherence. Jay decided to try another technique. He asked her about one of her favorite places to be, and she told him it was Hawaii. Jay pulled up some Hawaiian music and talked her through the coherence steps, and she was very soon able to sustain coherence. What is really amazing is that she had been refusing physical therapy treatments due to pain, but after her session with Jay, she was able to participate in a full PT treatment, with a smile on her face. The biofeedback readings below show the spike in coherence when her favorite music and memories were introduced.
cer. One of her goals is to get stronger to be able to tolerate a chemotherapy treatment regimen. The team’s new COTA, Jay, decided to try HRV training to reduce pain and increase function. During the first session, the patient was able to briefly get into what is called neurological coherence, as indicated on the biofeedback device as the green zone. However, the pain quickly brought her out of coherence. Jay decided to try another technique. He asked her about one of her favorite places to be, and she told him it was Hawaii. Jay pulled up some Hawaiian music and talked her through the coherence steps, and she was very soon able to sustain coherence. What is really amazing is that she had been refusing physical therapy treatments due to pain, but after her session with Jay, she was able to participate in a full PT treatment, with a smile on her face. The biofeedback readings below show the spike in coherence when her favorite music and memories were introduced.
 It’s easy to get caught up in the day-to-day routine in this line of work. You have new programs you want to start, financial markers you strive to hit, and all of this trickles down to your team. However, every so often, you are reminded of why you chose this profession. It’s the people, their stories, their lives, and all they share.
It’s easy to get caught up in the day-to-day routine in this line of work. You have new programs you want to start, financial markers you strive to hit, and all of this trickles down to your team. However, every so often, you are reminded of why you chose this profession. It’s the people, their stories, their lives, and all they share.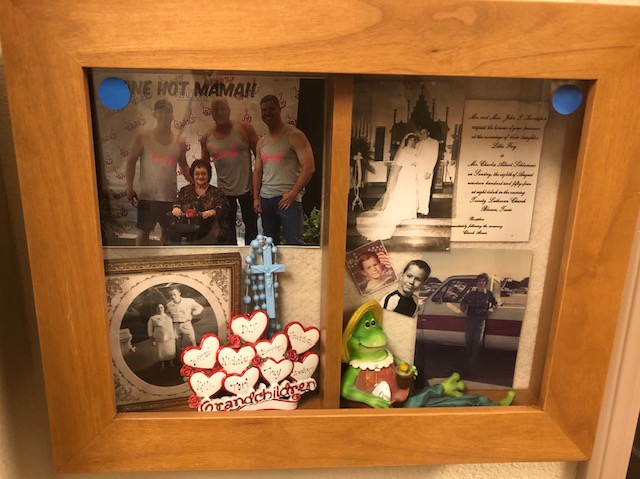
 Over the last year, Legend Oaks in New Braunfels, Texas, has implemented shadow boxes for all long-term care residents in an effort to decrease wandering, increase the patient’s ability to engage in meaningful interactions with other residents/staff/caregivers, and provide personalized, meaningful care in accordance with the patient’s Allen Cognitive Level. Residents were evaluated by a licensed therapist and determined if skilled therapy services were appropriate for the design and implementation of an FMP (Functional Maintenance Program).
Over the last year, Legend Oaks in New Braunfels, Texas, has implemented shadow boxes for all long-term care residents in an effort to decrease wandering, increase the patient’s ability to engage in meaningful interactions with other residents/staff/caregivers, and provide personalized, meaningful care in accordance with the patient’s Allen Cognitive Level. Residents were evaluated by a licensed therapist and determined if skilled therapy services were appropriate for the design and implementation of an FMP (Functional Maintenance Program). The patient’s Allen Cognitive Level was represented by color-coded dots on the outside of the shadow box, and the clinical staff, nurses and nurse aides received a three-week training course to increase their understanding of Allen Cognitive Levels and what each color represents. Examples of goals for the initial evaluation included:
The patient’s Allen Cognitive Level was represented by color-coded dots on the outside of the shadow box, and the clinical staff, nurses and nurse aides received a three-week training course to increase their understanding of Allen Cognitive Levels and what each color represents. Examples of goals for the initial evaluation included:


 Heart Math Variability, By Casey Murphy, Therapy Resource
Heart Math Variability, By Casey Murphy, Therapy Resource



 At Glenwood Care Center in Oxnard, CA, Cherryll Santos (L) and Aimee Bhatia (R) have a unique close relationship. Cherryll’s 18 years of leadership are evident in the culture of the nursing department, as this is a happy, cohesive team with strong clinical systems in place. Aimee, DOR, has been at Glenwood as a treating OT for five years, and a DOR for almost three. The relationship between these two leaders has a big impact on how nursing and therapy work closely together.
At Glenwood Care Center in Oxnard, CA, Cherryll Santos (L) and Aimee Bhatia (R) have a unique close relationship. Cherryll’s 18 years of leadership are evident in the culture of the nursing department, as this is a happy, cohesive team with strong clinical systems in place. Aimee, DOR, has been at Glenwood as a treating OT for five years, and a DOR for almost three. The relationship between these two leaders has a big impact on how nursing and therapy work closely together.